It may be like Neurologists, who are experts on the brain, but know nothing about Bartonella in the brain.
1. Infectious Diseases Practice Updates 2026
Lahaina, HI US
February 9, 2026 to February 13, 2026
*NO MENTION OF LYME, BABESIA OR BARTONELLA
https://ce.mayo.edu/sites/default/files/media/2025-10/ID2026%20Program-FINAL_1.pdf
2. Infectious Disease Boards
Large Infection Materials To Pass the Exam to be an “Infectious Disease Doctor.
They Have Trivial Education on Bartonella, Babesia, and Lyme. About a 1/2 hour of Study. Then You Are An Expert?
3. Infectious Conference
https://infectiouscongress.com/program/scientific-sessions/bartonella-infections
It mentions a short summary, but over 38 lectures that are not focused on Bartonella, Lyme, or Babesia.
They mention: Bartonella Infections
Among these, Bartonella henselae and Bartonella bacilliformis are notable [No. We find many species cause illness, including the early 90’s quintana that harmed WWI soldiers] for their association with diseases such as cat scratch fever and Carrion’s disease, respectively. [Bartonella lines 60,000 miles of human vessels and in my pending book we list over 50 symptoms and not the few with these two species!]
Bartonella species are primarily transmitted to humans through arthropod vectors, such as fleas, lice, and ticks, [We list at least 12 biting insect carriers from the published research] contributing to the complexity of their epidemiology. The manifestations of Bartonella infections range from mild, self-limiting conditions to severe, potentially life-threatening diseases [excellent point]. Cat scratch fever, for example, typically presents with fever, lymphadenopathy, [I see enlarged lymph nodes in 3% of positive patients] and skin lesions following a scratch or bite from an infected cat. Diagnosis of Bartonella infections involves various methods, including serological tests, polymerase chain reaction (PCR) [the best lab to do this is Galaxy Diagnostics and can detect it about 32%. If 3 draws on three days over a week the Bartonella can be detected in 93%]
However, the diverse clinical presentations and the challenge of cultivating Bartonella in laboratory settings can complicate accurate diagnosis. Treatment typically involves antibiotics, with choices depending on the specific Bartonella species involved. However, the chronic and persistent nature of some Bartonella infections, coupled with antibiotic resistance concerns, presents ongoing challenges in the management of these diseases.
They admit it is very hard to treat.
The CDC admits its treatment is not simple:
A number of antibiotics are effective against Bartonella infections, including tetracyclines [No. tetracyclines like doxycycline and minocycline only work in new acute settings], aminoglycosides, and macrolides. [True.] More than one antibiotic is often used. [Yes, since in the lab 3-4 treatments killed Bartonella best][No mention of biofilm. Bartonella is often coated with biofilm that makes these suggested treatments typically ineffective. Our #1 COMBATING BIOFILMS reference book has many to consider. We have been adding many biofilm options monthly since 2014.]
————————
Look at This Bartonella Blood Smear.
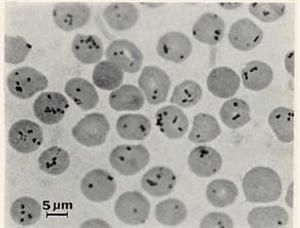
Does this look like it is cured in weeks with one or two of these antibiotics?
The Infectious Disease Society of America [IDSA]
They offer excellent treatment ideas for a thousand infections, but is this treatment of Bartonella exceptional? That would take 100-200 hours.
IDSA (Infectious Diseases Society of America)… recommend doxycycline or azithromycin as first-line treatments for Bartonella infections like Cat Scratch Disease (CSD) and Bacillary Angiomatosis (BA) [Doxy only kills in acute cases, per the leading expert Dr. Edward Breichwerdt, DVM with 200 research papers], often combined with rifampin, [Adding rifampin should be commonly used, not just with infected heart tissue. But it is profoundly more effective–rifabutin. After rifampin 600 mg am and pm is tolerated, we switch to rifabutin after an eye doctor rules out uveitis. Rifabutin has amazing tissue penetration. o because its ability to penetrate tissue very deeply is fascinating] …
[They add] …[We] will especially [use rifampin] for severe or invasive cases like endocarditis [heart infection], with treatment durations varying from weeks to months [Yes. At least] depending on infection severity and patient immune status. Extended courses (e.g., 3-4 months) and combination therapy [I doubt most infection doctors would typically do this. Maybe I am wrong. It happened in 1987. 🙂 Combinations of 3-4 treatments work best in lab studies and match the experience of elite physicians. And doxycycline is only for acute recent infection. They write: (doxycycline + rifampin) are common for severe manifestations, while shorter courses with azithromycin might suffice for milder CSD.
Conclusion
As I respect infection doctors, required to treat 1000 infections, it appears from their literature that this is not a priority. And some of their positions need to be revised to fit recent knowledge.
Any doctor can become an expert on an infection if they study 750-1000 hours.